

Picture the people who usually go looking for oxytocin. A mother sitting up at midnight, searching for anything that might help her autistic son connect a little more easily with his classmates. A couple who love each other but have gone quiet in the ways that used to feel easy, wondering if a nasal spray could soften the distance. Someone who struggles to trust the people closest to them and has read, somewhere, that a hormone could help with that too.
None of these are foolish reasons to be curious. They are, honestly, some of the most human reasons there are. And that is exactly why it matters what the actual research says, rather than what a product page implies. This piece walks through both: who tends to reach for oxytocin, what the science genuinely supports, and what a sensible, cautious next step looks like if you still want to try it.
Who this is really for
If you are hoping oxytocin will fix a relationship, calm a racing mind before a hard conversation, or help a child on the autism spectrum feel more at ease around other people, you are the audience this article is written for. You deserve a plain answer, not a marketing one. And the plain answer is layered: yes, oxytocin is a real hormone, no, most of what is sold about it is proven, and the difference between those two facts is where a lot of people get quietly misled.
Oxytocin (last reviewed here as of June 2026) is a small hormone your hypothalamus produces and your pituitary gland releases. Its two confirmed jobs have been known for the better part of a century: it drives labor contractions, and it triggers milk let-down during breastfeeding. That much is settled science, no asterisks needed.
The FDA-approved version, sold for decades as Pitocin, reflects exactly that narrow use. According to its FDA-approved labeling, oxytocin injection is used to start or strengthen uterine contractions during labor when medically necessary, and to control bleeding after delivery [P1]. It is given intravenously, in a hospital, by someone trained to watch for complications. That is the whole approved story. Nothing in that label mentions bonding, trust, calm, or intimacy, which turns out to be the single most important fact in this entire topic. Every time you see oxytocin marketed for those other things with a nod to its “FDA approval,” a quiet swap has happened: the approval belongs to childbirth medicine, and the promise being sold to you does not.
What the science actually says, claim by claim
I spent time this year working through the primary research rather than the product copy, and it helped to sort the claims by the person each one is aimed at.
For the person hoping to trust more easily. The origin story of the whole “love molecule” idea is a single 2005 experiment in which a puff of oxytocin made people more trusting in a money game. It made headlines everywhere. But when researchers later pooled the follow-up studies, the effect largely disappeared. A 2015 critical review in Perspectives on Psychological Science, led by Gideon Nave, concluded that the cumulative evidence “does not provide robust convergent evidence that human trust is reliably associated with” oxytocin [P2]. Larger, pre-registered replication attempts, the kind designed specifically to stress-test a shaky finding, failed to reproduce the original result. The claim that launched this entire category is the one its own field has walked back the furthest.
For anyone assuming the spray reaches the brain at all. This is the quiet structural problem sitting underneath everything else. For a nasal spray to change mood or behavior, enough oxytocin needs to travel from the nose into the brain to matter, and whether that happens is genuinely disputed among the people who study it. A 2016 paper in Biological Psychiatry, bluntly titled “Intranasal Oxytocin: Myths and Delusions,” found that “very little of the huge amounts applied intranasally appears to reach the cerebrospinal fluid” [P3]. What does reliably rise is oxytocin in the bloodstream, where it can act on the heart, gut, and reproductive tissue instead. If a seller talks about “topping up your brain’s oxytocin” as though that’s a settled mechanism, they are skating past a live scientific argument.
For the parent hoping it helps an autistic child connect. This is where the science was actually given a fair, rigorous test, and it matters more than any other single study here. In 2021, the New England Journal of Medicine published a phase 2 trial led by Linmarie Sikich: 290 children and adolescents with autism spectrum disorder, randomly assigned to either daily intranasal oxytocin at a target dose of 48 international units, or a placebo spray, for 24 weeks [P4]. Daily oxytocin did not significantly outperform placebo on the trial’s main measure of social functioning. This was not a small or casual study. It was built specifically to give oxytocin a real chance to prove itself, and on its central question, it did not.
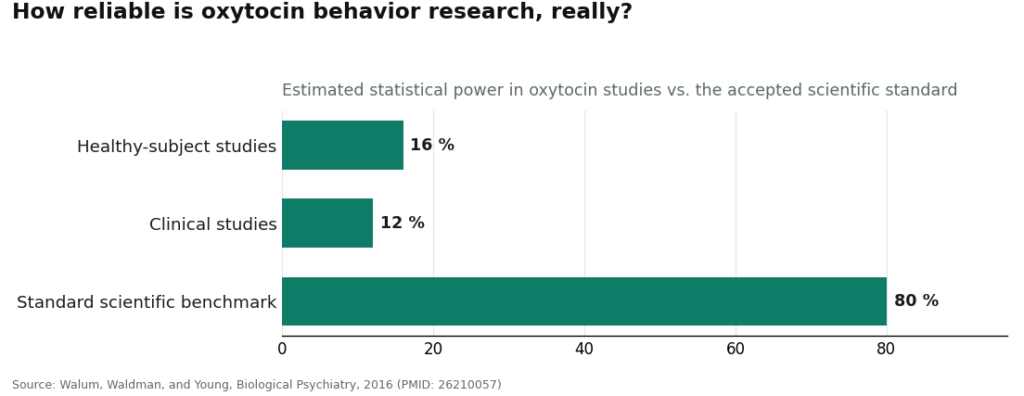
For anyone hoping a spray will simply calm them down or deepen a bond. Here the trouble isn’t a negative result so much as an unreliable one. Studies in this space tend to be small, results swing depending on the person and setting, and many celebrated positive findings have not held up under retesting. A 2016 methodological paper by Hasse Walum, Irwin Waldman, and Larry Young in Biological Psychiatry put an actual number on the problem [P5]. They estimated that the average oxytocin study in healthy adults had only about 16 percent statistical power, and clinical studies about 12 percent, against the usual scientific benchmark of 80 percent. Statistical power, in plain terms, is a study’s ability to detect a real effect if one exists. At those levels, real effects get missed, and a troubling share of the “significant” results that do get published are likely coincidences. The researchers’ own conclusion was that most reported positive findings on oxytocin and human behavior are probably false positives. That is not skepticism from outsiders. That is the field being honest about itself.
For the couple hoping it deepens intimacy. This is the one claim with a genuinely mixed record rather than a flatly disappointing one. A 2014 study in Hormones and Behavior, led by Behnia, gave couples intranasal oxytocin and found increased orgasm intensity and post-sex contentment, more noticeably in men [P6]. But the same study found no change in sexual drive or arousal on standard measures, and it was small. Other small studies have found no measurable change in how people consciously experienced sex at all. So this claim sits somewhere between “not nothing” and “nowhere near what the marketing suggests.”
What a “dose” even means here
If you read all of that and are still curious, it helps to know what “dose” actually refers to in this conversation, because it is not a wellness number, it is a research number. The only figure that comes from a large, carefully controlled human trial is the autism study’s 48 international units a day, split across the day, given intranasally under medical supervision [P4]. Worth sitting with: that is also the dose that did not beat placebo on the trial’s primary outcome.
There is no established, tested “bonding dose” or “calm dose,” because those uses were never proven in the first place. Any real number in the literature comes from a supervised research protocol, not a label on a vial that showed up in your mailbox. If you decide to move forward, this is a conversation for a licensed clinician who knows your health history, not a calculation to make alone from a forum thread.
How to actually go about it, if you decide to try
Say you have read all of this and you still want to try it. That is a reasonable place to land, as long as the decision that matters most gets made carefully: whether a licensed clinician is actually involved.
There are really only two paths here, and they do not resemble each other. One path runs through licensed telehealth. A clinician reviews your history, decides whether oxytocin is a reasonable thing for you specifically to try, writes a prescription if so, and a licensed pharmacy compounds and ships the product, with follow-up care built in. FormBlends works this way, and what that supervision buys you isn’t a promise that oxytocin will work. It’s a real person accountable for what’s in the bottle, and the same unvarnished honesty offered here: the popular uses are unproven and carry no FDA approval for anything beyond childbirth.
The other path is the gray market, where a vial marked “for research use only” arrives with no doctor involved anywhere, no prescription, and nobody responsible for what is actually inside it. The molecule in both vials might be chemically identical. Everything surrounding it is not. For a drug whose effects on the brain are still being argued over by the scientists who study it, that surrounding structure, the clinician, the pharmacy, the follow-up, is the part that actually protects you.
What is actually true, in one paragraph
Oxytocin is a real hormone with one solid, FDA-approved use: an intravenous drug for labor and postpartum bleeding [P1]. Past that, the popular story softens considerably. The nasal spray may barely reach the brain at all [P3]. The trust claim that started the whole “love molecule” idea has mostly failed to replicate [P2]. The largest, most rigorous trial in autism found no significant benefit over placebo [P4]. The wider literature on social behavior is so underpowered that its own researchers expect most positive results to be false [P5]. The intimacy research is a handful of small, mixed studies [P6]. None of that makes oxytocin fake. It makes the trendy claims unproven rather than disproven, which is a very different thing from what the marketing implies. A thoughtful person can still choose to try it, with realistic expectations and a clinician in the loop. Anyone promising you a guaranteed outcome is promising something the research simply does not contain.
Answers to the common questions
Is oxytocin nasal spray FDA-approved for bonding, calm, or intimacy?
No. The only FDA-approved form of oxytocin is the injectable used in hospitals to start or strengthen labor and control post-delivery bleeding [P1]. The nasal spray sold online for connection, anxiety, or sex is a compounded product, and none of those uses appear on any approved label. When a seller calls oxytocin “FDA-approved” while pitching it for bonding, they’re borrowing credibility from the childbirth drug for a use that has never gone through approval.
Does sniffed oxytocin actually reach your brain?
That’s genuinely disputed among the scientists studying it. A 2016 analysis in Biological Psychiatry found that very little of the oxytocin sprayed into the nose seems to reach the cerebrospinal fluid, even as blood levels climb sharply [P3]. That matters, because a spray can’t shift your mood through the brain if it’s mostly staying in your bloodstream. Treating brain delivery as an obvious fact skips over a real scientific argument.
Why did the trust claim behind the whole “love molecule” idea fall apart?
Because it didn’t survive rigorous retesting. A single 2005 study, where oxytocin made people trust each other more in a money game, launched the reputation, but a 2015 critical review found the pooled evidence doesn’t reliably tie human trust to oxytocin [P2], and later pre-registered replications couldn’t reproduce the original finding. The discovery that started this whole category is the one researchers have backed away from most.
Did oxytocin help autistic children in the largest trial ever run?
No. The strongest study in the field, a 2021 trial in the New England Journal of Medicine involving 290 children and adolescents with autism, gave daily intranasal oxytocin at roughly 48 international units for 24 weeks and found no significant improvement in social functioning compared to placebo [P4]. It was designed to give oxytocin every fair chance, and on its main outcome, it came up empty. Of everything covered here, this is the data point that should carry the most weight.
Is there a safe “wellness dose” of oxytocin nasal spray?
No validated dose exists for bonding, calm, or any wellness use, because those uses were never established in the first place. The one number from a large, carefully run trial is 48 international units daily, used in the autism study, and notably it’s also the dose that didn’t outperform placebo [P4]. Any legitimate figure comes from a supervised research protocol, not a mail-order label, so this is a question for a clinician familiar with your health, not something to work out from an online forum.
What’s the difference between licensed telehealth oxytocin and gray-market “research” vials?
The molecule can be identical, but the accountability around it isn’t. Through licensed telehealth, a clinician reviews your history, decides whether oxytocin makes sense for you, writes a prescription when it does, and a licensed pharmacy compounds and dispenses it with follow-up care, the model used by providers like FormBlends and the supervised tier behind names such as HealthRX. Gray-market vials labeled “for research use only” show up with no clinician, no prescription, and no one accountable for what’s actually in them. For a drug whose brain effects are still being debated, that supervision is the meaningful difference, not the price tag.
What does oxytocin nasal spray actually do when you use it?
Biologically, it delivers synthetic oxytocin to your nasal lining, and some enters your bloodstream. Whether meaningful amounts reach the brain circuits tied to bonding or calm is genuinely contested, as covered above. In controlled studies, its effects on mood, trust, and social behavior have been inconsistent and often modest. It doesn’t reliably produce the warm, connected feeling the marketing promises.
What are the known side effects of oxytocin nasal spray?
Reported side effects include nasal irritation, headache, nausea, and in some people a temporary rise in blood pressure. Because oxytocin affects uterine contractions, it carries real risk during pregnancy. Less commonly, some study participants reported more anxiety rather than less, which fits with research showing oxytocin can sharpen in-group and out-group divisions instead of simply soothing everyone. Long-term safety data for repeated intranasal use in otherwise healthy people is essentially nonexistent.
Is oxytocin nasal spray legal to buy?
In the United States, oxytocin is a prescription drug, so selling it without one is illegal. Vials labeled “for research use only” occupy a regulatory gray zone, but buying them for personal use still puts you outside FDA-sanctioned channels, and there’s no verification of what you’re actually getting. A compounding pharmacy working under physician supervision, the model FormBlends uses, is the legal, accountable route if a clinician decides it’s appropriate for you.
Where can you actually get oxytocin nasal spray, and what should you watch for?
Legitimate access runs through a licensed prescriber who sends a compounded formulation to a credentialed pharmacy. What shows up on supplement sites or research-chemical platforms is a different product entirely, with no guaranteed potency, sterility, or accurate labeling. In practice, that means you often don’t really know what you’re inhaling. If a website will sell it to you without ever asking for a prescription, that alone tells you something about how seriously they take your safety.
References
- Oxytocin injection (Pitocin), FDA-approved labeling: indicated for the initiation or improvement of uterine contractions to induce or augment labor when medically indicated, and to control postpartum bleeding; administered under medical supervision. DailyMed (U.S. National Library of Medicine). https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=dddcdcc3-cd4d-4573-98ac-9468bea23a8b
- Nave G, Camerer C, McCullough M. Does Oxytocin Increase Trust in Humans? A Critical Review of Research. Perspectives on Psychological Science, 2015;10(6):772-789. Concludes the cumulative evidence does not provide robust convergent evidence that human trust is reliably associated with oxytocin. https://pubmed.ncbi.nlm.nih.gov/26581735/
- Leng G, Ludwig M. Intranasal Oxytocin: Myths and Delusions. Biological Psychiatry, 2016;79(3):243-250. Concludes very little of the oxytocin applied intranasally appears to reach the cerebrospinal fluid while peripheral blood levels rise sharply.
- Sikich L, et al. Intranasal Oxytocin in Children and Adolescents with Autism Spectrum Disorder. New England Journal of Medicine, 2021;385(16):1462-1473. Phase 2, placebo-controlled trial of 290 participants; daily intranasal oxytocin (about 48 IU/day, 24 weeks) did not significantly improve social functioning versus placebo on the primary outcome.
- Walum H, Waldman ID, Young LJ. Statistical and Methodological Considerations for the Interpretation of Intranasal Oxytocin Studies. Biological Psychiatry, 2016;79(3):251-257. Estimates average statistical power near 16 percent in healthy subjects and 12 percent in clinical studies; concludes most reported positive findings are likely false positives.
- Behnia B, et al. Differential effects of intranasal oxytocin on sexual experiences and partner interactions in couples. Hormones and Behavior, 2014;65(3):308-318. Reported increased orgasm intensity and post-sex contentment, more pronounced in men, but no change in sexual drive or arousal.
Written by Ximena Ximenes, consumer-affairs writer. Reviewing the trials and labels directly. Last reviewed January 2026.
Nothing in this article is medical advice. Consult a licensed provider about your specific needs.